For full details about the dental benefits available from the DGA–Producer Health Plan, refer to the March 2025 Health Plan Summary Plan Description, beginning on page 91.
For a list of network dentists in your area, go to deltadentalins.com or call (800) 427-3237.
For Delta Dental coverage cards, call (800) 765-6003.
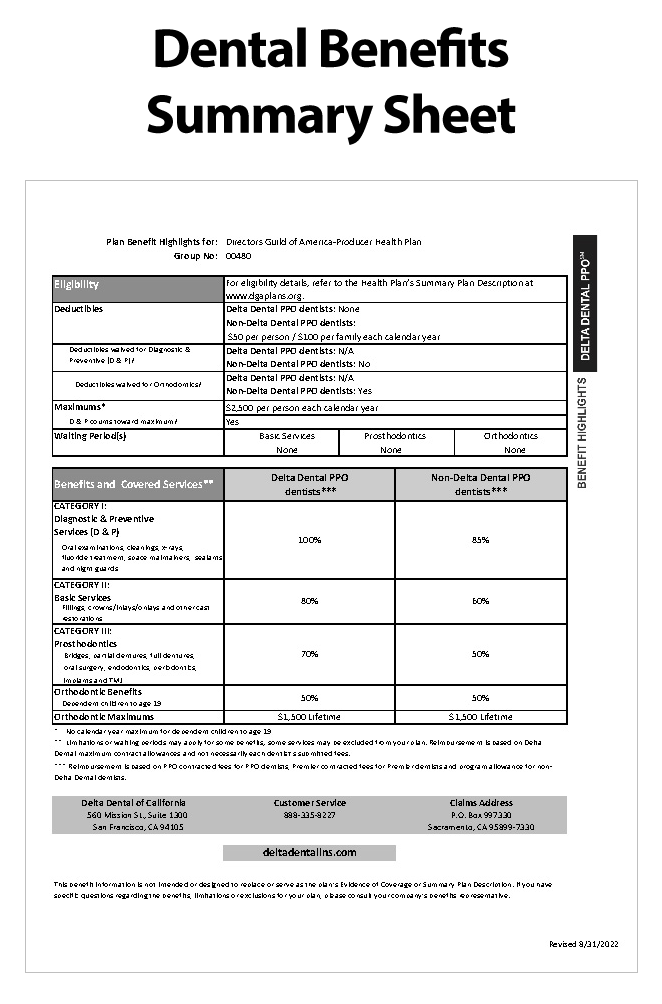
Below is a summarized schedule of dental benefits under the Health Plan.
| Network Dentists | Non-Network Dentists | |
|---|---|---|
| Calendar Year Maximum | $2,500 per person; Does not apply to children under age 19. | |
| Calendar Year Deductible | $0 | $50/person; $100/family |
| Co-Insurance (Category I) | 100% of covered expenses | 85% of covered expenses |
| Co-Insurance (Category II) | 80% of covered expenses | 60% of covered expenses |
| Co-Insurance (Category III) | 70% of covered expenses | 50% of covered expenses |
| Orthodontia | No deductible; 50% of covered expenses; Coverage only available for dependent children under age 19; Lifetime maximum payment of $1,500 per dependent child. | |
Delta Dental’s Wellness Library connects participants to dental resources all year long through relevant articles on topics, including dental care for cold and flu season, retainer care, and even the dental dangers of sports. Sort library articles by oral health categories to make finding new information and helpful reminders easy. Explore Delta Dental’s Wellness Library here.
Delta Dental’s educational webinars give participants the information they need to prioritize their oral health. Some engaging webinar topics include gum health and oral health. Click here to view future webinar dates and times or to register.
When you visit a Delta Dental dentist, your dentist should take care of your claim. However, if you go to a non-Delta Dental dentist, you will need to file your claim with Delta Dental.
The statement of treatment should include the dentist’s name, phone number, a description of each service the dentist performed, and the amounts billed and paid for each service.
…you can either call our office for the alternate social security number we assigned to you for identification purposes or enter your “Enrollee Number” which appears on your Delta Dental coverage card.
Mail your claim directly to Blue Cross at the address below:
Delta Dental
P.O. Box 997330
Sacramento, CA 95899-7330